
- Neuromonitoring
- Interview
- Reading time: 10 min
Multimodal monitoring in intensive care medicine: Advantages of measuring oxygen partial pressure (pₜᵢO₂)
Multimodal monitoring in neurointensive care can have a positive effect on patient outcomes. In an interview with RAUMEDIC, Prof. Oliver Sakowitz explains how measuring partial oxygen pressure (pₜᵢO₂) - in addition to ICP and CPP - can improve the detection of certain medical conditions.
Brief summary:
- Intracranial pressure (ICP) and cerebral perfusion pressure (CPP) are well-established parameters in neurointensive care.
- The additional measurement of partial pressure of oxygen (ptiO2) is a promising option. In the aftermath of a traumatic brain injury (TBI), for example, ICP and CPP alone are not sufficiently meaningful indicators for the early detection of ischemia.
- Multimodal neuromonitoring offers significant advantages compared to unimodal neuromonitoring and, scientifically well-founded, leads to better patient outcomes and a lower mortality rate. This is indicated by the results of the so-called 'Boost' studies.

Prof. Oliver Sakowitz
Professor Oliver Sakowitz, M.D., is Medical Director of the Neurosurgical Center Ludwigsburg-Heilbronn in Germany as well as Past President of the German Society for Neurointensive and Emergency Medicine (DGNI). RAUMEDIC had the opportunity to conduct an interview with the renowned expert on the role of oxygen partial pressure in the context of multimodal neuromonitoring.
In basic terms: what does multimodal neuromonitoring mean - and what is the difference compared to "regular" neuromonitoring?
In unimodal cerebral neuromonitoring, intracranial pressure (ICP) and cerebral perfusion pressure (CPP) are monitored. Multimodal neuromonitoring, or advanced cerebral neuromonitoring, involves the additional monitoring of other physiological parameters of the brain, such as the oxygen partial pressure (pₜᵢO₂) of brain tissue.
What exactly do ICP and CPP values indicate?
ICP measures the pressure inside the skull. CPP provides information about the pressure difference that is available for blood flow to the brain. The cerebral perfusion pressure is derived by subtracting the intracranial pressure (ICP) from the mean arterial pressure (MAP).
What fundamental advantages does multimodal neuromonitoring offer?
By simultaneously monitoring multiple parameters in addition to ICP and CPP, a more comprehensive picture of a patient's condition is obtained. This allows us as physicians to detect complications earlier, derive better and individualized treatment approaches, and ultimately make better treatment decisions.
Can you provide a specific example?
If oxygen partial pressure is monitored in addition to ICP and CPP, it allows for the analysis of tissue perfusion and oxygenation, which can lead to optimized treatment and better patient outcomes.
Can the advantage be explained in terms of a specific medical condition?
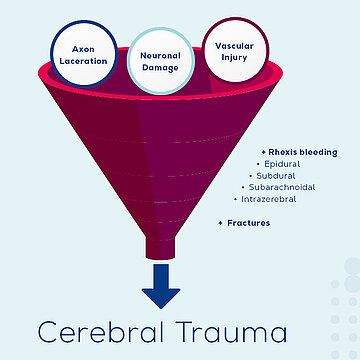
Certainly. In Germany, someone suffers from a traumatic brain injury (TBI) every 90 seconds, and a severe TBI occurs every 20 minutes. The problem, from a physician's perspective is that the clinical picture of TBI can be highly heterogeneous. With such a cerebral trauma, a variety of different injuries and damages to the brain can occur. These include neuronal damage, where nerve cells are affected, axonal injuries, which impact the nerve-cell extension, vascular injuries leading to bleeding in the epidural, subdural, or subarachnoid space or within the brain tissue itself, as well as fractures of the skull bones. The deeper a bleed affects the brain tissue, the more critical it is.
In this case, what role can multimodal neuromonitoring play in prevention?
By combining multiple monitoring parameters, an individualized assessment of the condition of the injured brain can be made. Additionally monitoring parameters such as ICP (intracranial pressure) and CPP (cerebral perfusion pressure), and also ptiO2 (partial pressure of brain tissue oxygen), can help prevent or detect early secondary damages associated with traumatic brain injury (TBI).
How do other brain disorders pose challenges for doctors in treatment?
Take, for example, an aneurysmal bleed. In addition to the primary damage caused by the bleed itself, secondary effects can also occur, albeit with a delay. There can be a gap of several days between a bleed and the occurrence of secondary harm. A typical example is vasospasm, a narrowing of the blood vessels in the brain, which impairs blood flow and can lead to reduced oxygen supply to the brain tissue, potentially causing ischemia in the affected area. Consequently, the brain tissue does not receive adequate oxygen and nutrients. This is precisely where the advantage of multimodal neuromonitoring can come into play.
Are ICP (intracranial pressure) and CPP (cerebral perfusion pressure) alone insufficient as indicators to detect conditions like ischemia early?
Cerebral oxygen deficiency—and the secondary brain damage associated with it—can occur even when ICP (intracranial pressure) and CPP (cerebral perfusion pressure) values are within normal ranges. This is because changes in cerebral oxygen supply or blood flow may only affect ICP and CPP values after a delay. The primary reason for this is cerebral autoregulation.
What does cerebral autoregulation mean as a challenge in neuromonitoring?
Mechanical (pressure-dependent) cerebral autoregulation is a compensatory mechanism designed to maintain adequate blood flow to the brain in cases of vessel constriction or reduced blood flow. The blood vessels adapt to maintain blood flow—regardless of fluctuations in mean arterial pressure (MAP). Remembering the calculation of cerebral perfusion pressure (CPP), with intact cerebral autoregulation, blood flow usually remains relatively stable, even with changes in CPP. However, with disrupted autoregulation, seemingly normal CPP values do not necessarily indicate normal cerebral blood flow!
Which parameter can be used to assess cerebral autoregulation?
The PRx value ("Pressure Reactivity Index") is suitable for assessing cerebral autoregulation. It is calculated as the correlation coefficient between ICP (intracranial pressure) and MAP (mean arterial pressure). The PRx value ranges between "+1" and "-1". A negative PRx value occurs when MAP increases and ICP decreases, indicating intact pressure autoregulation. Conversely, if MAP and ICP rise simultaneously, resulting in a positive correlation or PRx value, this indicates abnormal cerebral autoregulation, which can lead to negative neural outcomes.
What role do ptiO2 and cerebral vascular resistance (CVR) play in this context?
The healthy adaptability of the brain during regular cerebral autoregulation of blood flow ensures that the partial pressure of oxygen is maintained constant by adjusting to the cerebral vascular resistance (CVR). This keeps cerebral blood flow—and thus the partial pressure of oxygen (ptiO2)—largely independent of systemic blood pressure. However, this is not the case with dysfunctional autoregulation of blood flow.
What happens to CVR and ptiO2 during dysfunctional autoregulation?
CVR no longer responds appropriately to systemic blood pressure, and cerebral blood flow directly follows the fluctuations of systemic blood pressure. Consequently, ptiO2 can no longer be maintained constant through autoregulation and may experience significant fluctuations.
What exactly does the partial pressure of oxygen represent?
The partial pressure of oxygen in brain tissue reflects the availability of oxygen at a specific location at the cellular level. As a parameter, it expresses the balance between the oxygen delivery from the blood and the oxygen consumption of the brain tissue. It is influenced by changes in capillary blood flow, cerebral blood flow (CBF), and cerebral metabolism.
Does monitoring ptiO2 also impact patient outcomes, for example in patients with traumatic brain injury (TBI)?
The results of a retrospective cohort study from the USA in 2005 suggested this possibility. In this study, one cohort was treated with conventional ICP therapy. In the other group, ptiO2 was additionally monitored and included in therapeutic decisions. This approach led to a reduction in mortality and fewer discharges of patients to long-term care facilities. While the study was certainly not methodologically perfect, it indicates that the partial pressure of oxygen is an important parameter in neuromonitoring.
Could you elaborate a bit more on what has been examined in more recent studies?
In the "BOOST" study from 2017, researchers investigated whether there is a difference in the treatment of traumatic brain injuries when not only ICP (intracranial pressure) and CPP (cerebral perfusion pressure) are monitored but also ptiO2 (partial pressure of brain tissue oxygen). For this purpose, two groups or cohorts of patients were analyzed.
In one group, ICP and CPP were monitored and treated, while in the other, the ptiO2 value was additionally monitored. Both cohorts had roughly the same extent of pathological deviations in ICP and CPP values. However, there were significant differences in mortality rates between the groups: The mortality rate for patients treated with conventional ICP and CPP management was 34%. In patients where the partial pressure of oxygen in brain tissue was also monitored, the mortality rate was significantly lower, at 25%.
Is it therefore advisable to monitor multiple parameters through multimodal neuromonitoring - regarding patient outcomes?
In view of positive treatment outcomes, it is desirable to be able to monitor multiple parameters for in neurointensive care. It is encouraging that the understanding of the benefits of multimodal neuromonitoring is increasingly becoming established in hospitals.
Prof. Sakowitz, thank you very much for these fascinating insights and your time!
You're welcome, thank you too!

Let’s connect
